Smaller Doses, Smaller Footprint: How Low-Dose HIV Prevention Could Cut Costs and Carbon

Daniel Kiesa
As the HIV prevention landscape evolves, the number of biomedical options is growing. New drugs like long-acting injectables and novel oral agents promise to expand choice, improve adherence, and reach new populations. But one factor may have an outsized influence when it comes to real-world access: cost.
For antiretroviral (ARV) products, it is widely understood that the single biggest cost driver is the active pharmaceutical ingredient (API), the molecule that blocks HIV. The math behind API cost for HIV prevention is straightforward but powerful: how complex is the API to manufacture, and how much API is needed to deliver protection?
Some ARV APIs are relatively simple to make. Others, especially newer classes like capsid inhibitors, require complex chemistry, specialized inputs, or longer production cycles. This complexity makes early production expensive, sometimes costing thousands of dollars per kilogram. Over time, process innovation and manufacturing scale can reduce costs, but even the most efficient production can only go so far if large doses are required. That is where dose size becomes an important factor.
Once a product completes trials and gains regulatory approval, its required dose is largely fixed. While formulation, packaging, and distribution all contribute to price, the amount of API per dose becomes a fixed cost multiplier.
Let’s compare the annual API requirements for different HIV prevention options:
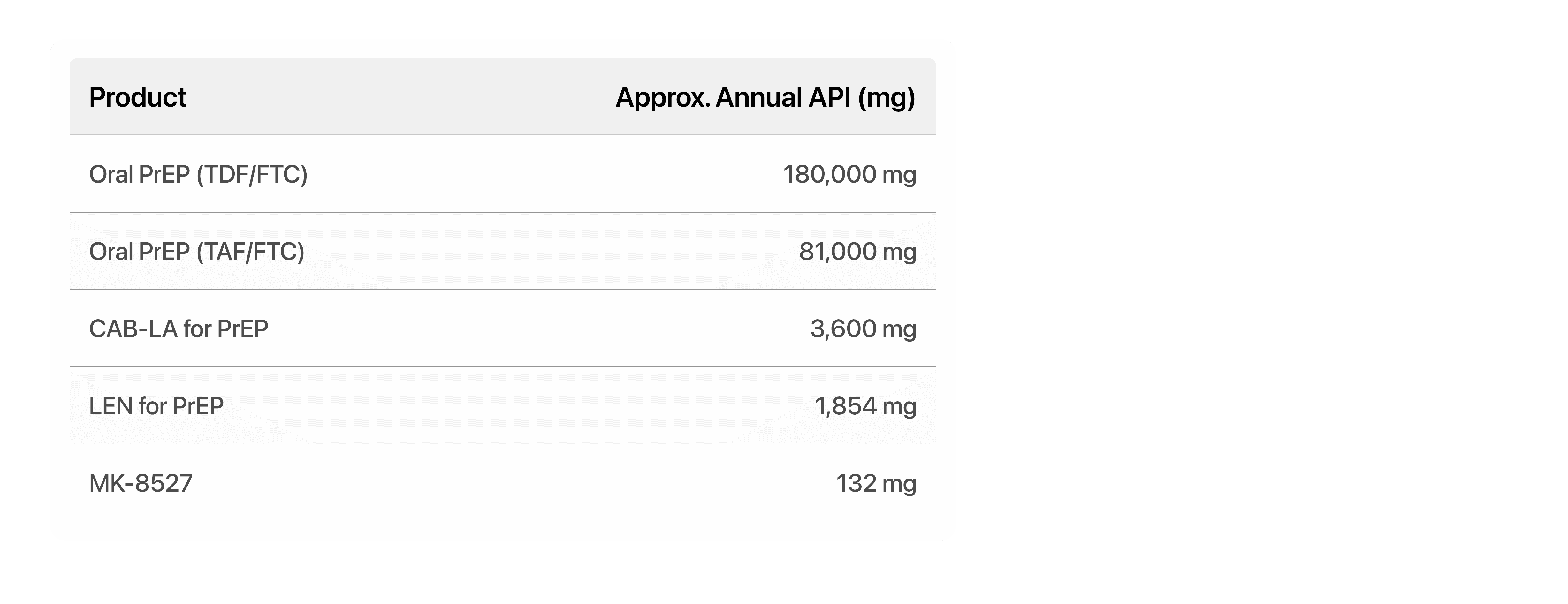
In the race to expand HIV prevention, some of the biggest breakthroughs might come in the smallest doses.
Cheaper, Local, and Greener
API cost and complexity are half the equation. The amount of API required per year is the other half, and it has major implications for affordability, local manufacturing, and environmental sustainability.
Once a medicine is proven, API mass per year becomes one of the strongest predictors of its potential for cost reduction. Smaller doses mean less raw material, lower transport weight, and smaller production footprints, all of which drive down costs over time. When evaluating new PrEP options, stakeholders should look beyond efficacy and delivery convenience to the milligrams per dose, because that is where affordability begins.
HIV treatment drugs are among the most widely produced medicines in the world. Historically, production has relied on large-scale batch manufacturing suited to high-dose APIs such as the 600 mg daily Efavirenz regimen. Low-dose medicines, by contrast, are often inefficient to produce using the same infrastructure. But they open doors to new technologies such as continuous or flow manufacturing, which are better suited for smaller-volume, high-value products. As manufacturers modernize production equipment, there is an opportunity to locate facilities closer to end users, building local or regional capacity. Low-dose products could be the entry point for sustainable, distributed manufacturing models in Africa and other regions.
The environmental dimension of dose size is often overlooked. API production is a major driver of the carbon footprint for antiretrovirals, largely because of the high energy demands and solvent use associated with chemical synthesis. Lower-dose regimens can significantly reduce the emissions associated with manufacturing, packaging, and logistics. For instance, smaller quantities of raw materials translate directly into reduced chemical waste, lower energy consumption, and fewer transport emissions.
In addition, oral solid dosage forms tend to have greater stability, avoiding the need for cold-chain or refrigerated transport. They can be stored and shipped at ambient temperatures, using standard containers rather than energy-intensive refrigerated ones. Compact packaging also allows more doses to fit into smaller spaces, reducing both storage costs and freight emissions. When scaled across millions of users, these efficiencies could represent a meaningful reduction in the carbon footprint of global HIV prevention programs.
Lower-dose products therefore offer a triple win: they can be more affordable, easier to produce locally, and better for the environment.
Conclusion
As the next generation of HIV prevention products moves toward rollout, the amount of API in each dose may be one of the simplest yet most powerful predictors of real-world access and sustainability. The shift toward lower-dose regimens has the potential to transform not just cost structures but entire supply chains. Smaller, more efficient production can support local manufacturing, diversify supply sources, and strengthen regional resilience.
This evolution is also an opportunity to align global health priorities with broader goals of sustainability and equity. A lower-dose future means a smaller environmental footprint, reduced reliance on global transport, and increased opportunities for local industry participation.
In the end, cost is not only about price tags and procurement budgets. It is about the efficiency, adaptability, and fairness of the systems that deliver medicines to people who need them. As HIV prevention options multiply, paying attention to the milligrams in each product could help determine how far our investments can go – financially, operationally, and environmentally. Sometimes, the smallest details can make the biggest difference.
References
MSF Access Campaign, Untangling the Web of Antiretroviral Price Reductions; Clinton Health Access Initiative (CHAI) ARV market reports.
Clinton Health Access Initiative, HIV Market Report (2023). Price of TDF API <$100/kg reported based on market data.
TDF = 300 mg/day, FTC = 200 mg/day → combined 500 mg/day × 365 days = 182,500 mg/year (rounded to 180,000 mg). See WHO Prequalification Dossier or FDA labeling for Truvada.
TAF = 25 mg/day, FTC = 200 mg/day → 225 mg/day × 365 = 82,125 mg/year (rounded to 81,000 mg). See Descovy FDA label.
CAB-LA dosing is 600 mg every 8 weeks after two initiation doses (total: ~3,600 mg/year). Source: ViiV Healthcare product information and HPTN 083 trial protocol.
Lenacapavir (LEN) for PrEP is being studied at ~927 mg every 6 months = 1,854 mg/year. See: Gilead press releases, CAPELLA & PURPOSE 1 trial designs.
